Editor’s note: Dave Chase is the CEO of Avado.com, a patient portal and relationship management company that was a TechCrunch Disrupt finalist. Previously he was a management consultant for Accenture’s healthcare practice and founder of Microsoft’s $2 billion health platform business. You can follow him on Twitter @chasedave.
Healthcare has long been a technology paradox. There have been few places further out on the cutting edge of technology than biotech and medical devices. In contrast, healthIT has been in a time warp (see Why It’s Good News HealthIT is So Bad). Nearly 20 years after the advent of the web, the dominant healthIT vendors have thrived on a business model and technology architecture that harkens back to when Wang and Prodigy were cutting edge. That is, most healthIT still has the same company provide technology from the top to the bottom of the stack.
Healthtech Investors Double Down
The widespread use of the web disconnected the front-end, user-experience technology supplier from the back-end. Whether it’s travel apps or package tracking, consumers are able to tap into back-end systems without knowledge of what mainframe or client-server system may be running those systems. The spike in digital health investment reported by Rock Health’s Q3 2012 Funding Report echoes what I heard from hospital executives at two recent healthtech-related conferences – Health 2.0 and the Digital Health Conference. That is, for the first time in my experience, these executives talked about how they recognize that they have a flood of new requirements and they have zero expectation that their legacy healthIT suppliers will meet those needs in the next 2-3 years.
This projection is due to legacy vendors being overloaded with their core business (e.g. installing electronic health records) and also having slow product cycles. Healthcare executives explicitly talk about how they want EHR-agnostic tools that will work with their EHRs. Increasingly, providers recognize that while they have complained about vendor lock-in strategy reminiscent of the Wang era, the risk of lock-in increases exponentially if they also adopt consumer/patient-facing tools from their legacy vendors. It’s one thing to disrupt your staff with switching EHRs, it’s quite another to ask patients to switch tools as well. Smart providers are disconnecting those two decisions like virtually every other industry already has. This dynamic is the core reason for the New York Digital Health Accelerator (NYDHA). See Rip Empson’s article here on why the NYDHA was formed and has 22 large healthcare providers engaging with startups at a level that is unprecedented in healthcare. [Disclosure: My company, Avado, is one of the eight companies selected for this program.]
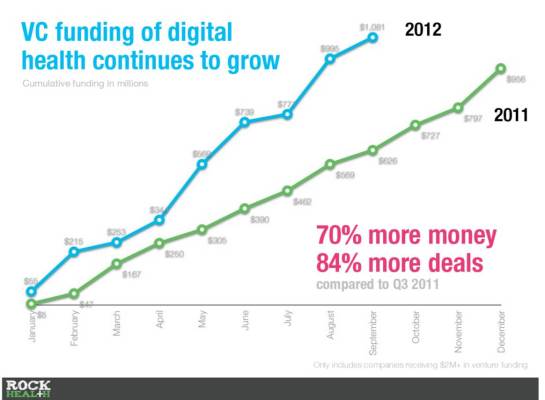
The following slide deck from Rock Health highlights key findings such as an increase in dollars invested by VCs of 70 percent and 84 percent more deals over a year ago:
Growth in healthtech investment isn’t limited to the U.S. For example, noted investors/entrepreneurs Esther Dyson, Peter Frishauf (founder of Medscape) and Milena Adamian (founder of Life Sciences Angel Network – New York) recently invested in the Series A for VitaPortal in Russia. It’s also not limited to traditional VCs as we saw in a Community Hospital Joins Wave Of New Strategic Venture Funds To Drive Disruptive Innovation.
Legacy Health IT Built For The Last Battle
Already healthcare providers are realizing that what they thought was going to be their 100 percent solution is really best optimized for just 25 percent of where healthcare dollars are spent (hospital-based care). In reality, 75 percent of healthcare spend is directed toward chronic disease. Legacy healthIT has its strength in automating internal workflows of hospitals and other clinical settings. In those high-intensity settings, healthcare providers make the decisions that drive the patient health outcomes. However, with chronic disease, it’s an entirely different story. The decisions that individuals (or their families) make drive the health outcomes. For example, does the patient fill a prescription and take it properly? Or do they make the necessary lifestyle choices to optimize their health?
This dynamic isn’t lost on thought leaders in healthcare. One of the leading thinkers in healthIT, Shahid Shah (aka The Health IT Guy), laid out why legacy EHRs are ill-prepared for the era of accountability that is rapidly transforming healthcare.
The EHR systems and IT required for MU (Meaningful Use) is a quite different from what will be required for ACOs,” Shah continued. “It will be nowhere as easy for existing legacy EHRs to simply retool their current platforms, like they did for MU.”
With that said, Shah outlines nine ways future EHRs need to support ACOs.
1. Sophisticated patient relationship management (PRM). According to Shah, today’s EHRs are more document management systems, rather than sophisticated, customer/patient relationship management systems. “For them to be really useful in ACO environments, they will need to support outreach, communication, patient engagement, and similar features we’re more accustomed to seeing, from marketing automation systems than transactional systems.”
Read full article here.
Health Systems Making Newspaper Industry Mistakes
Despite a clear recognition of the radical transformation that is happening, it is striking that the path many healthcare providers are taking parallels that of newspaper companies (another local oligopoly/monopoly that had barriers to entry that were no longer unassailable). See WWJD? The CEO Every Healthcare Leader Should Learn From for more. In contrast, providers such as those in the NYDHA are taking a different path.
In the above piece, newspaper executive John Paton had a three-point prescription for reinvention that led to a 5x revenue increase and halving of capital expenses. This resulted in his organization going from bankruptcy to $41 million in profit in two years. There were three keys to his approach that can be applied by healthcare leaders:
- Speed to market: One new product launched per week (See Related Article: The Rise of Nimble Medicine)
- Scaling opportunity: Sourced centrally, implemented locally. Ideas can come from all over. Identify the best ideas/people from all over.
- Leverage partners: Feed the firehose of ideas from outside. This is at the heart of why astute healthcare executives in New York have actively engaged in an accelerator that is without precedent.
Unfortunately, most newspapers didn’t adhere to that prescription. It’s a cautionary tale for hospitals, in particular. In other countries when the shift happened from a reactive “sick care” system to a proactive health-focused system, over half of the hospitals closed. Naturally, forward-looking hospitals and health systems are making moves to not only survive, but also to thrive.
New York Is A Harbinger Of Things To Come In Healthcare
If you want to see the future of healthcare, New York is a great place to start. Nirav Shah, MD, MPH is the New York State Commissioner of Health for the State Department of Health. Dr. Shah talks about fundamentally rebuilding the healthcare system. The stakes are high to make that happen. Dr. Shah oversees a budget of over $50 billion that has 5 million Medicaid recipients. Like all states, they see healthcare’s hyperinflation is devastating state budgets and education budgets, in particular (see Bill Gates TED Talk for more). “The old system, acute care focused in the hospital. That was the past. Tomorrow is chronic disease focused in an outpatient setting. That is what the Health Home program promises and that is what the Medicaid program is investing in. That is what the NYDHA is all about.” The pace of decisions by NYDHA providers is dramatically faster than procurement models of the past. I’ve already seen one Health Home program (and the hospital that is running it) evaluate and make a selection in less than two months. For those of us familiar with the excruciating year-plus decision processes of the past that has crushed many a startup, this is exciting.
At the kick-off event for the NYDHA, Intel veteran and current Executive Director of the New York eHealth Collaborative (NYeC), David Whitlinger discussed that the health information exchange his organization operates (the State Health Information Network of New York – aka the “SHINY”) will allow software developers to facilitate the information exchange critical to reinventing healthcare delivery. The missing link has been having tools that sit on top of the SHINY. The NYDHA startups will get first access to their APIs and then it will be opened more broadly.
In order to achieve those goals, it’s critical to have the right resources and players at the table. Maria Gotsch, president and CEO for the Partnership for New York City Fund, is building off of the tremendous success of the FinTech Innovation Lab that her organization orchestrated for healthcare. The NYDHA is intended to foster innovation and economic development. In tandem with the NYeC, Gotsch’s organization got commitments from 22 large healthcare providers and seven investment funds to deeply engage with the program.
For a long time I said “healthcare is where tech startups go to die,” as the decision processes in healthcare favored 20-30 year old companies that could wait out excruciatingly convoluted decision processes. Those decision processes not only killed many startups, they doomed healthcare providers to outdated technology and price tags reminiscent of the mainframe era. But times have changed.
At a recent presentation given by Leonard Achan, RN, MA, ANP and chief communication officer for the prestigious NY-based Mount Sinai, described how they have changed how they worked in the past and contrasted to what they are doing now. He said that that they are far more open to working with startups. Rip Empson reported on one example of this. Just a year ago, who would have thought mainstream healthcare organizations would be releasing “app stores” of their own. This is why VCs are voting with their pocketbooks on healthcare’ reinvention fueled by breakthrough startups leaving the Wang/Prodigy era behind.